Early in the pandemic it became evident that widespread testing would be a vital tool to control COVID-19. People infected with SARS-CoV-2, the virus that causes COVID, can shed the virus and infect others for some days before they become sick. It’s not enough to isolate people with fever and a cough: you need to catch them before they even know they are sick. Additionally, more than half of infected, and therefore infectious, people never have symptoms or know that they are sick.
Read more
This story is a sidebar to the article "Healthy Davis Together: Could This Be the Future of Public Health in America?"
But in the first few months of 2020 in the U.S., tests were expensive and hard to get, especially after the first test kit distributed by the Centers for Disease Control failed to work properly. Even if you could get a test, it could take up to two weeks to receive your results.
Simple, inexpensive and quick
A team at the UC Davis Department of Pathology and Laboratory Medicine, working with the Center for Immunology and Infectious Disease on campus and the California National Primate Research Center, developed their own diagnostic test for SARS-CoV-2 based on samples from the first patient treated at UC Davis Medical Center — also the first known U.S. case of COVID-19 in someone who had acquired it in the community, rather than from foreign travel. But this test was intended for clinical use with patients, not for community screening. Like most COVID-19 tests, it also involved the infamous “brain scrape,” with a swab deep in the nasal cavity.
Testing was slow, expensive and hard to get, but all of us have done PCR in our labs.” — Ken Burtis, professor of molecular biology
Once that swab is taken, the test is based on a PCR or polymerase chain reaction. PCR is a widely used technique for making multiple, identical copies of a single, specific piece of genetic material (DNA or RNA).
“Testing was slow, expensive and hard to get, but all of us have done PCR in our labs,” said Professor Ken Burtis, a molecular biologist who came out of retirement to serve as chief operating officer of Healthy Davis Together, or HDT, up to May 2021.
Back in early 2020, Burtis began talking with Richard Michelmore, professor of plant sciences and director of the UC Davis Genome Center, and they started to explore possible routes to developing a homegrown test for asymptomatic screening.
“We needed in-house testing to be able to bring students back to campus,” Michelmore said. To be workable, the tests needed to be simple to take, as inexpensive as possible and to deliver results quickly — preferably within 24 hours.

Turning up the volume
Diagnostic tests used in hospitals prioritize sensitivity — detecting virus in a patient at the lowest possible level, increasing time and costs. But community testing of people without symptoms could use a slightly lower sensitivity test. Indeed, high sensitivity might be a drawback, leading to false positive results or chasing down people who had nearly cleared the infection and were no longer a risk to others.
Michelmore has spent much of his career fighting pandemics — in plants. The world’s food crops are constantly threatened by diseases, such as stem rust in wheat, he said.
“Plant pandemics probably kill more people, through starvation and malnutrition, than COVID,” he said.
Michelmore could see that hospital labs aiming at hundreds of samples a day would be overwhelmed by the volume of testing required for widespread screening. But he knew that the agricultural biotech sector was using technology that could run many times more samples than medical center labs could.
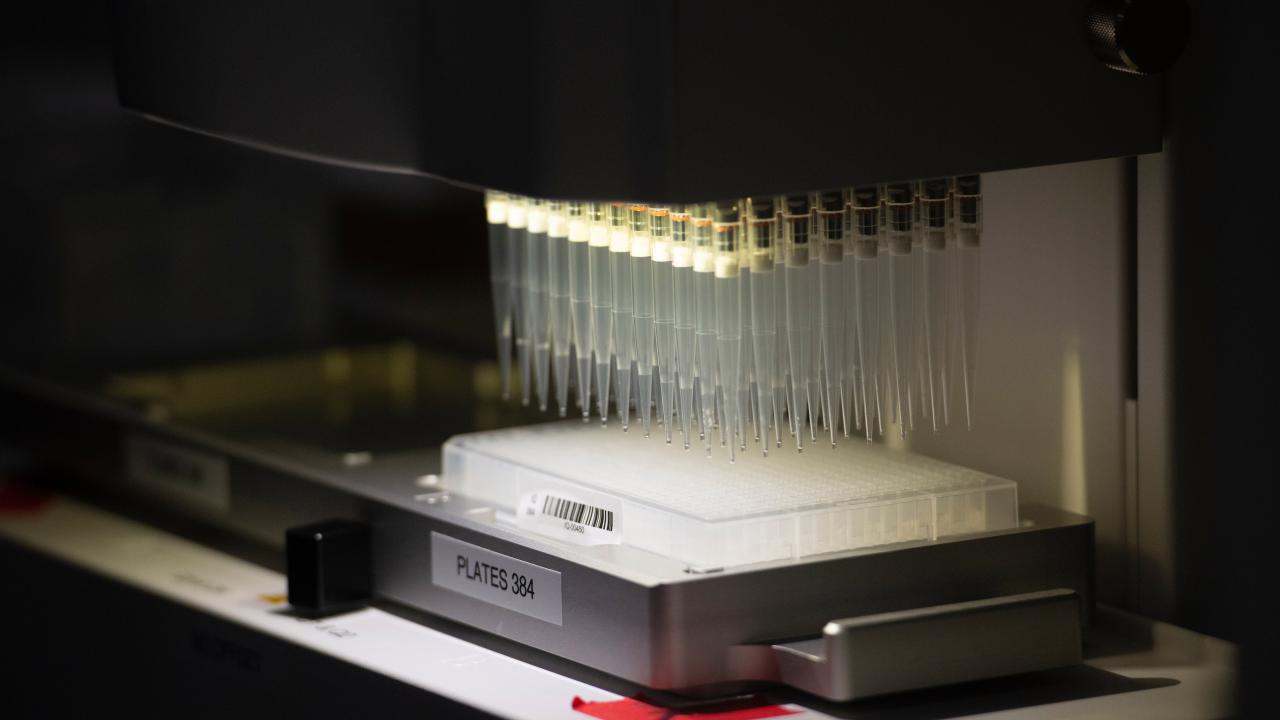
Michelmore and colleagues began talking with companies, first with Corteva Agriscience and then LGC Biosearch. The team consequently proposed in-house testing based on purchasing IntelliQube robotic PCR machines from LGC Biosearch. These machines can run thousands of samples per day in tiny wells.
Saliva over swabs
To make taking the test easier, the team wanted to use saliva rather than nasopharyngeal swabs. But saliva is viscous and does not play nicely with robotic microwell technology. Lutz Froenicke, manager of the DNA Technology core at the Genome Center, came up with the idea of using the enzyme papain — also known as meat tenderizer — to pre-treat the samples, making them fluid enough for easy processing.
Saliva samples are collected in barcoded tubes. That barcode means that the Genome Center lab can test a sample and send the results to the Student Health Center (for on-campus samples) or to HDT (off-campus samples), which matches the barcode to an electronic health record for the patient. The Genome Center never sees any personally identifying information.
In early August 2020, Provost Mary Croughan approved purchase of an IntelliQube and ancillary equipment for up to a million dollars, with a goal of being able to test all students who returned to campus in mid-September six weeks later. A second machine was purchased later through HDT.
Down to the last detail
More challenging than the test itself was designing the process for collecting samples and handling the data. There were many details to decide, from the number and location of collection kiosks and nearby parking, to the best method for collecting saliva and whether UC Davis could buy enough barcoded tubes to collect samples.
Setting up the testing program involved people from across the campus, from purchasing and HR to parking services and IT, Michelmore said. “It’s been a massive, massive team effort and it happened extremely fast.”
Michelmore especially credited Kelly Ratliff, vice chancellor for finance, operations and administration, for driving the effort from the top and Dr. Cindy Schorzman, medical director at Student Health and Counseling Services, for coordinating the diverse campus elements and overseeing the complex medical aspects.
“People really stepped up,” he said.